

Primary Care Doesn't Need Saving. It Needs Re-Architecting.
The fix for primary care is not more staff, more pay, or more grit, but a new operating system.

A comment on a Doximity thread last week did more diagnostic work than most healthcare op-eds. In response to my previous post “AI will displace physicians. The only question is the order.” another physician responded:
“Well, maybe AI will figure out that primary care sucks too.”
That comment is the whole problem stated in fifteen words.
It is also the start of the answer.
For two decades the conversation about primary care has centered on staffing shortages, reimbursement compression, and burnout. All three are real. None of them are the architecture.
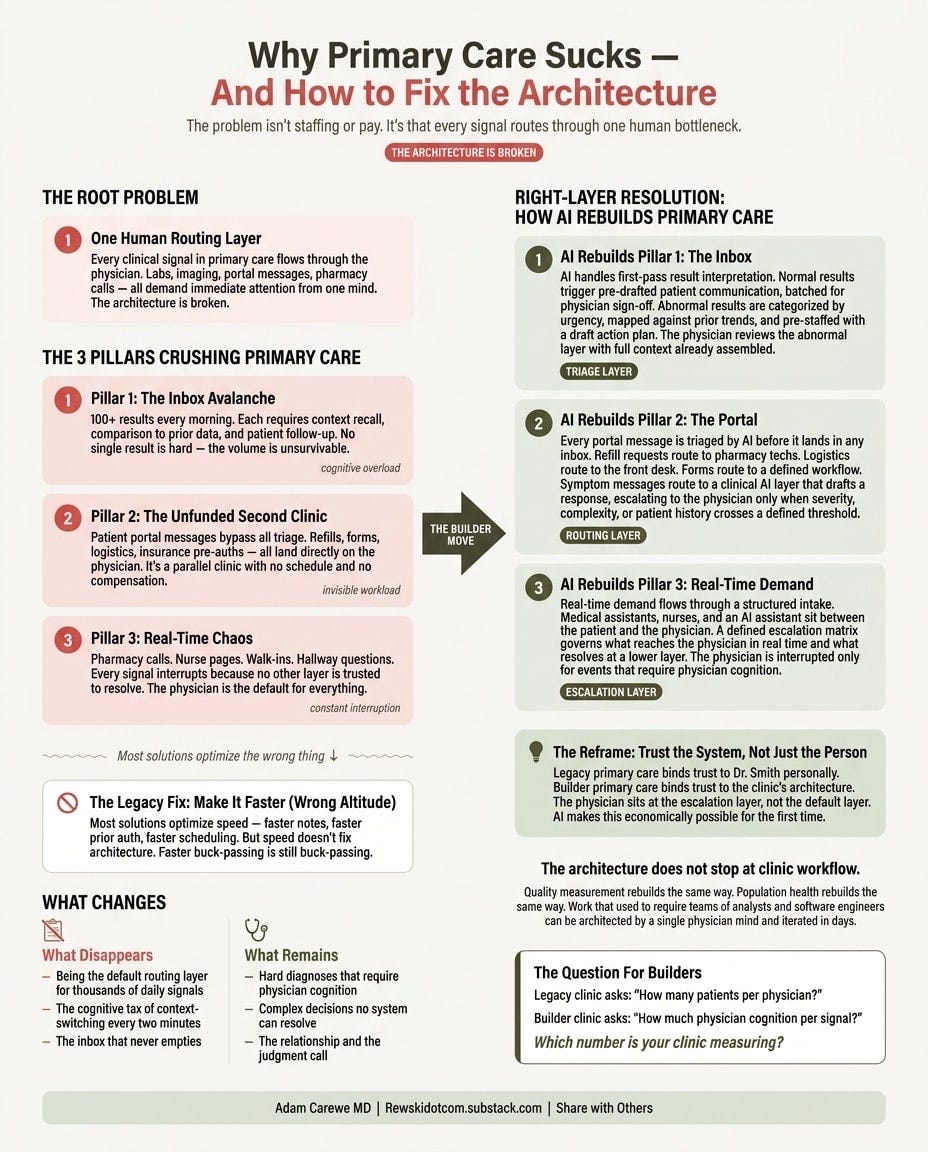
The architecture is this. Every clinical signal in a primary care clinic routes through one human bottleneck. The physician.
The Three Pillars Crushing Primary Care
Pillar 1: The Inbox.
A primary care physician opens her chart at 7 a.m. and sees a hundred results. Lab panels. Imaging reads. Specialist notes. Each one demands context recall, comparison to prior, decision on action, and a message back to the patient. No single result is hard. The aggregation is unsurvivable. The cognitive load is not the result. It is the volume routed to one mind.
Pillar 2: The Portal.
Patients message their physician directly. Most of those messages should never reach a physician. Refill timing. Appointment logistics. School notes. Form completions. Insurance pre-authorizations. The portal was sold as access. It became an unfunded second clinic running in parallel to the first, with no schedule, no staffing model, and no compensation structure.
Pillar 3: The Real-Time Demand.
Phone calls from pharmacies. Pages from nurses. Walk-ins. Hallway questions. Each arrives without warning and demands an answer now. The current model handles real-time by interrupting the physician mid-task. The physician is the default routing point because no other layer has been built. Every signal escalates because no other layer is trusted to resolve.
Three pillars. One root cause. Primary care binds every clinical signal to a single human routing layer.
The Reframe: Trust Is In The System, Not The Person
Legacy primary care binds trust to a person. The patient trusts Dr. Smith. Dr. Smith carries every signal personally because she is the trust contract.
Builder primary care binds trust to a system. The patient trusts the clinic’s architecture. The physician sits at the escalation layer, not the default layer. She shows up for the cognition that genuinely requires a physician. Everything else resolves at the right altitude before it reaches her.
This is not a staffing change. It is not a workflow tweak. It is an operating system change. AI is the substrate that makes this architecture possible at primary care economics for the first time.
Faster Is Not The Reframe
Most of the industry is trying to make legacy primary care faster.
Faster note-writing. Faster prior auth. Faster scheduling. Faster refills.
That work is not wrong. It is just at the wrong altitude.
Faster note-writing assumes the note should still be written by the physician. The builder question is different. Why is the physician writing the note at all? Build a system that writes the note for you. I have not written a note in my practice in eighteen months. General Medicine is a 50-state national practice. The note is generated, structured, and signed. The physician’s cognition is spent on the patient, not on the documentation that proves the visit happened.
The same logic decomposes every legacy pain point. The legacy primary care workflow runs on pass-the-buck. The phone rings. Someone answers, takes a note, hands it to the next person. That person reads it, resolves it, or hands it to the next person. Each handoff is a layer of latency and a layer of dropped context. The signal moves through a chain of partial reads before anyone with enough authority and information closes the loop.
This is a paper-days problem the digital era inherited. Orders went onto paper. We flipped a flag on the binder. A clerk pulled the chart and transcribed the orders. When something was unclear, the clerk asked the nurse to clarify, because the doctor had already moved on. The nurse resolved it. That part of paper actually worked. The nurse was reachable. The signal closed at the layer that could close it. Then Epic and the EMRs that followed digitized the flag and the rack. They did not preserve the nurse-resolution loop. They hard-coded the buck-passing without the practical wisdom that made it survivable. Two decades later, pass-the-buck is the default architecture inside the largest EMRs on the market.
The builder move is a three-layer resolution architecture.
Real-time resolution. The right person with the right authority closes the signal the first time it lands. No handoff.
Asynchronous resolution. Signals that can wait route to a defined queue with a defined response window. The patient knows when to expect resolution. The clinician knows when the work happens.
Scheduled resolution. Signals that belong inside a visit route to a visit, with full context pre-assembled before the visit starts.
A clinic that resolves every signal at the correct layer the first time sings and hums. A clinic that passes the buck through three or four hands per signal burns out its physicians and frustrates its patients, no matter how fast each handoff becomes.
Faster handoffs are the legacy optimization. Right-layer resolution is the builder move.
What Primary Care Should Actually Do
Pillar 1 rebuilt. AI handles first-pass result interpretation. Normal results trigger pre-drafted patient communication, batched for physician sign-off. Abnormal results are categorized by urgency, mapped against prior trends, and pre-staffed with a draft action plan. The physician reviews the abnormal layer with full context already assembled. Result review time drops sharply. The cognitive tax drops further because the mental model arrives pre-built.
Pillar 2 rebuilt. Every portal message is triaged by AI before it lands in any inbox. Refill requests route to pharmacy techs. Logistics route to the front desk. Forms route to a defined workflow. Symptom messages route to a clinical AI layer that drafts a response, escalating to the physician only when severity, complexity, or patient history crosses a defined threshold. The physician sees a curated, pre-drafted, pre-prioritized queue. The portal becomes a routed channel, not a parallel clinic.
Pillar 3 rebuilt. Real-time demand flows through a structured intake. Medical assistants, nurses, and an AI assistant sit between the patient and the physician. A defined escalation matrix governs what reaches the physician in real time and what resolves at a lower layer. The physician is interrupted only for events that require physician cognition. Everything else resolves at the layer where it should have been handled all along.
The pattern across all three. AI is not replacing the physician. AI is decomposing the cognitive load so the physician shows up for the work that requires her.
What disappears: the cognitive tax of being the default routing layer for every clinical signal in the clinic.
What remains: the cognition that actually requires a physician. The hard diagnosis. The complex decision. The relationship. The judgment call that no system can resolve.
The Joy Returns When The Architecture Holds
The Doximity comment was right. Primary care sucks right now. It does not suck because the work is bad. It sucks because the architecture asks a physician to absorb every signal in a system that produces thousands of signals a day.
When the architecture holds, the work changes. The physician sees the patient she is supposed to see. She reads the result she is supposed to read. She makes the decision she is supposed to make. The thousand unmarked intersections that currently demand her attention resolve at the layers that should have been handling them all along.
This is what System C looks like at the front line. Industrialized medicine routes every signal through the physician because that was the only available architecture (and the reimbursement machine.) Integrated intelligent scalable care routes signals to the right layer, with AI as the operating system that makes the routing economically possible at primary care scale.
And the architecture does not stop at clinic workflow. Quality measurement rebuilds the same way. Population health rebuilds the same way. Work that used to require teams of analysts and software engineers can be architected by a single physician mind and iterated in days. That is the part that is untouchable in legacy bedrock. The legacy stack cannot move at that speed because it was never designed to.
None of this is theoretical. For the last eighteen months I have been building this clinic in real time. Not as a thought experiment. As a working national practice. There is more to share as the system matures. This is the first piece of that story.
The headlines say AI is coming for primary care.
The reality is that AI finally makes primary care possible.
The Question For Builders
The legacy clinic asks how many patients per physician.
The builder clinic asks how much physician cognition per signal.
If you are still measuring the first number, you are operating in System B.
If you are designing for the second, you are building System C.
Which number is your clinic measuring?
This resonates deeply, especially the distinction between routing every signal through the physician versus reserving physician cognition for the decisions that actually require it.
Feels like many of the current economic and workflow failures stem from conflating those two things.
This framing is very close to the real issue: primary care is not just understaffed; it is under-architected.
More clinicians, more grit, or more documentation automation may help temporarily, but the deeper failure is that patients, clinicians, staff, referrals, follow-ups, and unresolved context still move through systems that were never designed to preserve shared operational awareness.
AI can help, but only if it becomes part of a better care operating model rather than another layer placed on top of the same broken handoffs.